This is an a online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
A 24 year old male daily wage labourer came to the OPD with a chief complaints of decreased urine output, shortness of breath and vomitings since 4 days.
HOPI
Patient was apparently asymptomatic 8 days back then he developed severe vomitings due to an excessive binge drinking without any consumption of food. The vomitings were non bilious, non blood stained, non foul smelling, watery and occurred immediately after consumption of food or liquids.
Patient developed oral ulcerations later that day. He was taken to a local hospital where medication was provided. 4 days ago he had complaints of shortness of breath (Grade 4) and decreased urine output with blood in the urine. On taking him to a local hospital, dialysis was advised after which he was admitted to our hospital. 2 days ago the patient was observed to develop a white coating in the mouth and over the tongue( dermatology opinion taken).

He has no H/o fever, loose stools, pedal oedema, burning micturition, cough
Past history:
No similar complaints in the past
No H/o HTN, diabetes, asthma, epilepsy and tuberculosis.
Personal history:
Diet: mixed. Appetite: decreased
Bowel and bladder: irregular.
Sleep: adequate. Addictions: alcohol and paan.
Allergies: none. ( binge drinking episode. Daily
80ml. )
Family history: not significant
General examination:
Patient is conscious coherent and cooperative moderately built and nourished
Vitals
Temperature: afebrile. PR: 83bpm
RR: 22cpm. BP: 140/90mmHg
Pallor: absent
Icterus: present

Cyanosis: absent
Clubbing: absent
Lymphadenopathy: absent
Oedema : absent
Systemic examination:
Per abdomen: soft on palpation, bowel sounds heard, no distention present


Respiratory system: no wheeze heard, no crepitus heard, normal vesicular breath sounds heard
CVS: S1 S2 heard, no additional murmurs
CNS: no focal neurological deficits
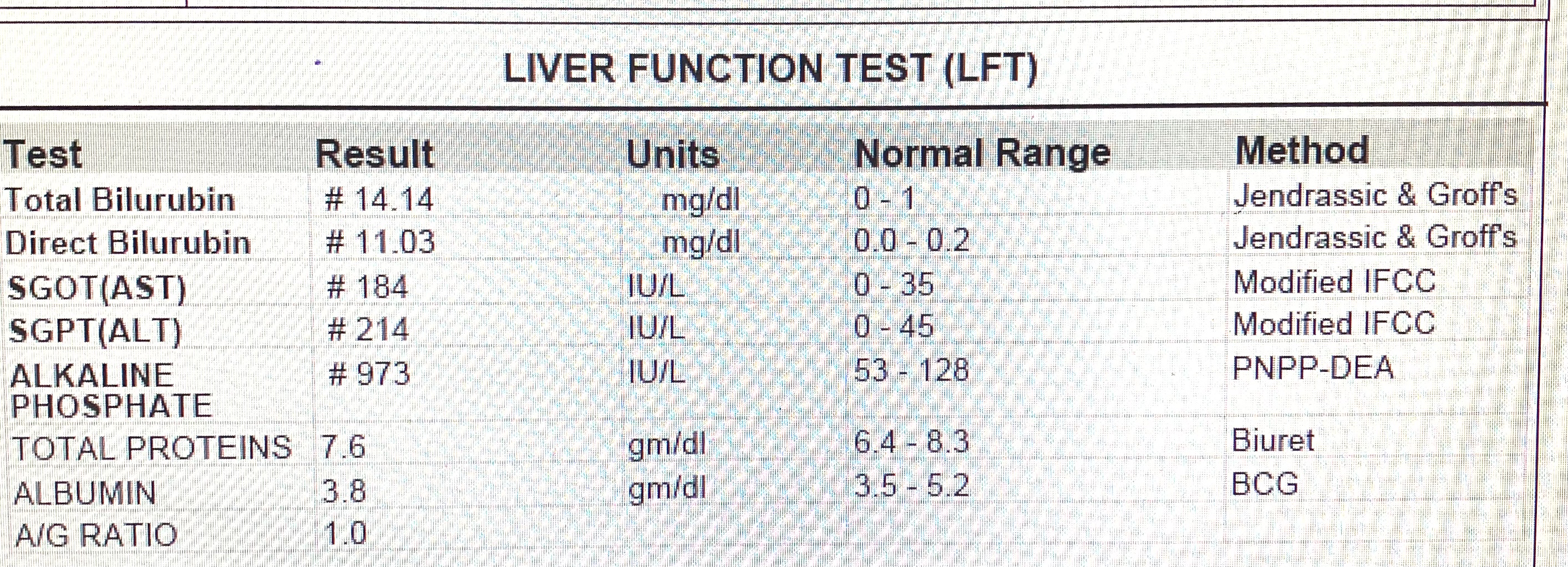
Investigations:







Chest CT
Provisional diagnosis: Alcohol liver disease ,Acute kidney injury, aspiration pneumonia, oral candidiasis.
Treatment:
- IV NS
- Inj zofer (SOS)
-Inj Doxycycline 100mg BD
- Inj Thiamine 200mg in 100ml NS TID
- Inj Monolef BD
- Inj Lasix 40mg BD




No comments:
Post a Comment