55 year old male hailing from nalgonda , farmer by occupation presented to our casuality in post cardiac arrest- intubated state on 5th march at 4:27pm
HOPI


●Not a known case of HTN,DM,ASTHMA,STROKE
PERSONAL HISTORY
●Non vegetarian consumes pork meat with normal appetite,regular B&B movements
● No known allergies ,smoker and alcholic for the past 20 years and no history of weight loss
Family history
● h/o seizures in both of his grand children
examination

Rx
1. Head end elevate 30•
2. Inj . MEROPENEM 1gm/IV/BD
3. Inj.LEVIPIL 500mg / IV/ BD
4.Inj. Mannitol 100ml/IV/BD
5.Inj. MIDAZO LAM 10mg - 50 mgNS (@ 3ml / hr)
6.Inj. Pantop 40mg/IV/OD
7. Inj.Neomol 100 ml/if temp >101.5•
8.RT feeds —-100 ml with nills
(2 hourly ) 100ml with free water
9. Vitals monitoring hrly
10.Fever chart Hourly
11.Inj.thiamine 2AMP in 100 ml ns/iv/bd
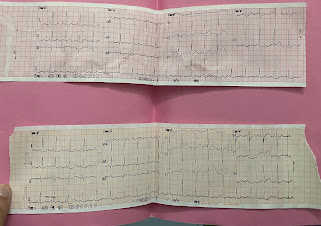
● Ecg taken on day 1

■ Investigations done -








Rx
1. Head end elevate 30•
2. Inj . MEROPENEM 1gm/IV/BD
3. Inj.LEVIPIL 500mg / IV/ BD
4.Inj. Mannitol 100ml/IV/BD
5.Inj. Pantop 40mg/IV/OD
6. Inj.Neomol 100 ml/if temp >101.5•
7.RT feeds —-100 ml with nills
(2 hourly ) 100ml with free water
8. Vitals monitoring hrly
9.Fever chart Hourly
10.inj Monocef 1gm/iv/bd
11.Inj.thiamine 2AMP in 100 ml ns/iv/bd
Investigations-




● Diagnosis - seizures 2• to ? tuberculoma/NCC
? Alcohol
With hypoxic encephalopathy, post cpr status day 6, mechanical ventilation day 5
■ Day 3 soap notes
O/E patient is on mechanical ventilator
Gcs- E1 V M2
Fever spikes+
Rx
1. Head end elevate 30•
2. Inj .MIDAZOLAM 10mg in 50ml ns @3ml/hr
3. Inj.LEVIPIL 500mg / IV/ BD
4.Inj. Mannitol 100ml/IV/BD
5.Inj. Pantop 40mg/IV/OD
6. Inj.Neomol 100 ml/if temp >101.5•
7.RT feeds —-100 ml with nills
(2 hourly ) 100ml with free water
8. Vitals monitoring hrly
9.Fever chart Hourly
10.inj Monocef 1gm/iv/bd
11.Inj.thiamine 2AMP in 100 ml ns/iv/bd
Advised 2D echo
Investigations-


● Diagnosis - seizures 2• to ? tuberculoma/NCC
? Alcohol
With hypoxic encephalopathy, post cpr status day 7, mechanical ventilation day 6
Fever chart

















No comments:
Post a Comment